Successful together in dentistry and dental technology
Become a DIR® Partner in a strong network
Are you looking for a strong partnership in the field of functional diagnostics with a closed anamnesis and therapy principle that can be easily integrated into your daily practice/laboratory routine?
Then you will find DIR® user and become part of the DIR® community and benefit from the advantages of the targeted use of the DIR® concept.
Your advantages as a DIR®partner:
Innovative technologies: Use our advanced solutions and services to provide your patients with the best possible care.
Professional training: Get access to exclusive education and training to keep you and your team on the cutting edge of functional diagnostics.
Strong market positioning: Benefit from our extensive marketing support to optimally position your practice/dental laboratory as a leading provider in functional diagnostics.
Network: Become part of a network of experts and gain early access to new products and developments.
Cooperation based on trust: Our partnership is based on trust and long-term cooperation.
We support you every step of the way.
How to become a DIR®Partner:
Contact us: Fill out our contact form or call us right away.
Consultation: In a personal consultation, we will clarify all the details and provide you with comprehensive information about the possibilities of a partnership.
Training and induction: We offer you comprehensive training and induction so that you are optimally prepared.
A joint start: After the qualification, we start together with the implementation of your individual strategy and the integration of our systems in your practice/dental laboratory.
Please contact us:
Would you like to find out more about the possibilities of a partnership?
Contact us today using the contact form below – we will be happy to advise you!
Transparent results for exact positioning data of the mandible, temporomandibular joints and muscles and the basis for perfect prosthetics
Every dentist wants a theoretically “exact bite” in which the physiological position of the temporomandibular joint is achieved at the moment the bite is taken.
In practice, however, this is almost never the case, as the patient is only ever able to provide the actual situation of their bite – especially due to the daily varying influences that the patient and dentist are naturally subject to.
This “bite registration in the actual situation is therefore often the basis for any further dental findings and any subsequent dental work.
It can therefore lead to undesirable problems in the dental ⁄ dental reconstruction.
In most cases, massive grinding measures and corrections are then necessary.
The DIR® system offers the dentist extensive possibilities for a perfect basis for all types of diagnostics and all “bite-based” work.
If the correct procedure is followed, it is generally no longer necessary to make any corrections in the patient’s mouth. Apart from the ease of carrying out a digital jaw relation determination, the DIR® system provides immediately evaluable and comprehensible images of the patient’s current ACTUAL situation.
With the proven DIR® coding principle under defined masticatory force, you also receive an exact bite for perfect prosthetics at all times – independent of the dentist.
The electronic measuring method is based on the arrow angle or support pin registration according to Gerber with recording of the marginal movements of the mandible under physiological masticatory pressure and without reference to occlusion.
Centric position as target bite
Once the DIR® measurement has been completed, the centric position determined is encoded in the patient’s mouth as a so-called target bite by inserting the support pin into a fixation plate under defined chewing pressure and injecting or scanning silicone between the rows of teeth.
This is then transferred to the articulator (analog or digital).
DIR® Sensor
The patented in-house development for recording the movement sequences of the lower jaw and the chewing force exerted.
DIR® measuring amplifier
The measuring amplifier transmits the data to the DIR® System software in real time.
DIR® positioning unit
The latest stepper motor technology for faster and almost noiseless control of the determined encryption position.
The calibration function implemented in the software ensures convenience and maximum precision.
Medical PC
21.5˝ Slim design Multi-Touch Medical Panel PC 16:9 Full HD, Windows 10, touchscreen, front IP65
Medical Tablet
9.7″ multi-touch medical panel tablet 4:3, Windows 10, touchscreen, front IP65 Docking station
DIR® Software
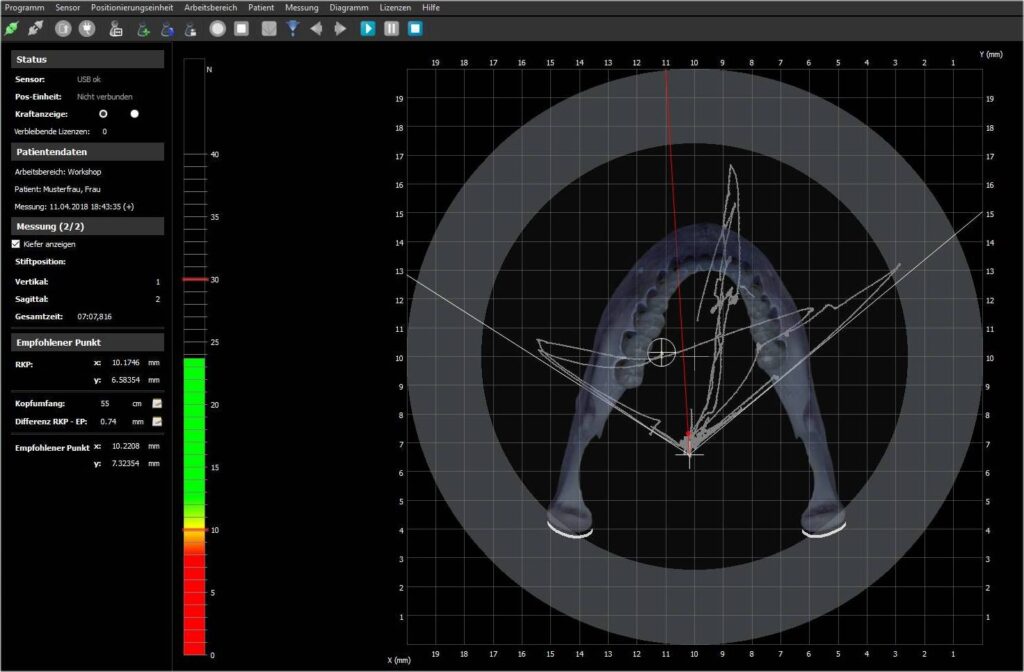
The software records the measured sensor values received from the measuring amplifier via the USB interface, which are linearized and geometrically corrected in order to display the force application point.
It is displayed on the screen in an X-Y coordinate system.
The total force determined is also shown on the display as a vertical value bar and serves as biofeedback for the patient to maintain the optimum range of jaw muscle force during registration.
DIR® suitcase trolley
Sturdy and custom-made transport trolley case for safe transportation of the DIR® System measuring unit
Your dentist is not only responsible for your teeth
If your symptoms indicate CMD: Talk to your dentist about functional disorders!
An optimally functioning craniomandibular system (jaw, temporomandibular joints, teeth, chewing muscles) is a prerequisite for the health of the entire organism.
This quickly becomes apparent in the case of functional disorders or CMD (craniomandibular dysfunction).
Various, sometimes painful complaints can occur.
You should go to the dental practice if symptoms such as pain in the temporomandibular joints or in the face, head and neck area as well as symptoms such as teeth grinding, jaw clicking, headaches, ringing in the ears or tension along the spine remain unexplained.
With the help of manual-clinical and instrumental functional diagnostics, dentists can find a reliable diagnosis – the first step towards ending your suffering!
This is your way: Find YOUR® dentist!
Not all functional diagnostics are the same: The DIR® concept with scientifically proven treatment methods and state-of-the-art medical technology is only offered by dentists who are qualified to do so.
We therefore recommend the following procedure:
1. if you want to stay with the dentist you trust…
Are you experiencing the symptoms described above, but no doctor or therapist has been able to find the cause?
Contact your dentist now!
Ask him or her about functional diagnostics with the DIR® concept (FunktioCheck Pro® / DIR® system) at your next appointment.
2. if you are flexible and would like to see an experienced DIR® dentist…
Use the online dentist search to find a DIR® dentist near you or contact the “Gesellschaft für Funktionsdiagnostik” directly.
The clinical picture of CMD (craniomandibular dysfunction) describes the pathological condition of a functional disorder or mechanical misload of the masticatory muscles.
The clinical picture also includes the connective tissue supporting the masticatory muscles (fascia, tendon) with secondary dysfunction and damage to the temporomandibular joints, teeth, periodontium and, more rarely, the soft tissues of the oral cavity when biting the cheeks, tongue or lips.
According to current knowledge, the clinical picture must be extended to include functional disorders/damage to the neck, nape and (with restrictions) also the back muscles and the associated spinal joints.
Functionally healthy versus dysfunctional
According to epidemiological studies, around six percent of the European population live functionally healthy lives, whereas the prevalence of objective findings of CMD without evidence of subjective complaints is 85 percent.
According to this, a large proportion of the population is confronted with triggering disruptive factors and reacts with progressive and/or regressive tissue adaptations.
These structural changes can be neuronally compensated or tolerated for years and remain clinically inconspicuous in the sense of a silent CMD.
Only around nine percent of the population have developed full CMD with persistent objective and subjective symptoms.
In this group, tolerance to the disruptive factors has been lost and, as a result, the neuronal ability to compensate has collapsed.
Women more frequently affected than men
In a gender comparison, women are affected by CMD around five times more frequently than men, with the peak age being between 30 and 34 years.
The prevalence values of typical CMD complaints also increase dramatically when symptoms such as tension headaches, migraine complaints, neck and back pain, ringing in the ears or tinnitus, hearing loss, balance disorders, dizziness, swallowing difficulties, speech and taste disorders, which were previously not primarily attributed to “dental diseases” but to diseases from other specialist areas (see above), are included in the evaluation.
CMD-triggering disruptive factors
The evaluation of the relevant specialist literature regarding the etiology of CMD reveals four triggering disruptive factors, which makes the multi-causality or multifactorial genesis of the disease clear.
The following causes are described in detail, which can of course also occur in combination:
Dento-occlusal interference factors
Traumatic surgical disruptive factors
Orthopaedic disruptive factors
Psychosocial disruptive factors
Dento-occlusal interference factors
Dento-occlusal interference factors and traumatic-surgical interference factors fall into the specialist areas of dentistry, oral and maxillofacial surgery, pediatrics, speech therapy, orthopedics and manual medicine.
Dento-occlusal interference factors are classified as pre- and postnatal developmental defects of the teeth and acquired diseases of the teeth and periodontium, including periodontal remodeling processes and factors caused by dental intervention.
They therefore relate to malocclusions after tooth migration or tilting or due to sliding obstacles, supraocclusions during elongation or early contact, non-occlusions or infraocclusions due to tooth loss and tilting, incorrect jaw relationships with condyle displacements due to forced occlusions or incorrect bites for prosthetic restorations and orthodontic, conservative and prosthetic treatments.
Dental interventions during jaw and muscle growth of the two dentitions can cause much more extensive damage than corresponding treatments in adults, whose bone and muscle tissue can only be remodeled to a limited extent, due to the still pronounced biological ability of the developing organism to adapt its shape.
The problem of iatrogenic orthodontic treatment errors lies in the influence on the natural tooth angulations, whereby corrections to the axial position of the upper first molar represent the greatest risk factor for a dento-occlusal disorder, because the 6-year molar influences the angulations of all replacement and growth teeth that erupt after it, with the exception of the anterior teeth.
Therefore, the leveling of Spee’s curve, which is the aim of the straight-wire technique, must be considered a treatment error in the legal sense.
Traumatic surgical disruptive factors
The traumatic surgical disruptive factors relate to mechanical injuries and maxillofacial surgery on the jaws (especially on the ascending branch and the condyle), the teeth, the temporomandibular joint and the spinal joints as well as the associated musculature, resulting in changes in size, shape and position as well as underdevelopment (e.g. condylar asymmetries) after wound healing is complete.
Orthopaedic disruptive factors
The orthopaedic disruptive factors are located in the specialist fields of orthopaedics, manual medicine, pediatrics, speech therapy, dentistry and oral and maxillofacial surgery.
They relate to pre- and postnatal developmental defects and acquired diseases of the bones, joints and muscles of the spine with resulting postural or positional defects of the cervical spine, including developmental defects and acquired diseases of the jaws, temporomandibular joint, masticatory muscles and tongue (e.g. as growth inhibition due to thumb sucking habit resulting in persistent infantile swallowing) as well as orthopaedic surgical interventions on the spine.
Psychosocial disruptive factors
Psychosocial disruptive factors are naturally assigned to the fields of psychiatry and psychology.
Surprisingly, only very few studies have been published that deal with the question of the epidemiological distribution or demographic frequency of the named disruptive factors.
However, there is current data on the increasing dominance of psychosocial disruptive factors over the last few decades.
The mechanisms by which psychosocial stress (as a synonym for disruptive factors) can contribute to the development of CMD were described by Gameiro et al.
in a review.
According to this, stress can profoundly modulate the processes of pain conduction and perception in the sense of a psychosomatic projection (somatization or somatoform disorder).
Furthermore, bruxism and compressio dentalis (teeth clenching) can be seen as a sign of a stress management strategy and serve to protect against chronic stress-related illnesses.
The non-physiological increase in teeth grinding and clenching can be convincingly explained by Lazarus and Laurier’s transactional stress model, according to which each person has individual stress coping skills (active and passive coping).
In active coping according to the frustration-aggression theory, the aggressive reaction occurs on a somatic-muscular level as an archaic fight response.
In the passive coping strategy, frustration triggers resignation and subsequently depression.
Parafunctions
Just like the psychosocial stress factors, the three other disruptive factors also generate neuronally controlled muscle hyperactivity or hypertonization of the masticatory muscles with a lack of rest phases, which is defined by the term parafunctions and triggers primary structural and functional damage to the musculature.
These are then the cause of secondary consequential damage to the temporomandibular joints, periodontium, teeth, adjacent soft tissues, neck muscles and cervical spine joints.
Do you know what it’s like: grinding your teeth, clenching your jaw? Noises in your ears?
Complaints in the head, neck and spine area?
Did you also know that even headaches, sleep disorders and even tinnitus can have their cause in the jaw?
Are you one of those people who frequently suffer from one or more of these complaints but have not yet received a concrete diagnosis from doctors and therapists?
Then you are not alone!
There is often a malfunction of the lower jaw and jaw joints (craniomandibular dysfunction or CMD) with a “wrong bite” as a result of dysregulation, which in turn can trigger complaints throughout the body.
If you are affected, ask a specialist specializing in functional diagnostics whether you have a functional disorder.
You can use our dentist search to find DIR® dentists in your region.
Incorrect bite and CMD
Bite disorders and CMD with the symptoms described are widespread.
They are functional disorders of the craniomandibular system (jaw, jaw joints, teeth, masticatory muscles).
However, the causes can be not only functional, but also structural, biochemical or psychological (e.g. teeth grinding due to stress).
The most important functions of the craniomandibular system are chewing and speaking: Functions that we need all the time.
If there is a functional disorder, chewing and speaking, even laughing, leads to persistent overload, which can then trigger painful stress symptoms throughout the body.
A vicious circle
More than 1,500 dental contacts every day – about half of them at night – are a real challenge for your teeth.
Every person with a fully edentulous jaw has a “stress protection system”.
This stress protection system is not only used for speaking, laughing and swallowing, but also during physical activity.
If the stress protection system is disturbed by insufficient or increased tooth contact – e.g. due to incorrectly positioned crowns or old fillings – the bite is no longer optimal.
Receptors report these incorrect or interfering contacts to the brain.
The brain in turn sends the message to the masticatory muscles: Bite down harder – correct the misalignment!
The increased strain leads to overloading and pain in the neck and chewing muscles and spreads to the entire body.
The physical complaints mentioned above often occur as a possible consequence of the dysfunction.
Malfunction?
The figures speak for themselves: around 10% of the population are affected by misalignments of the temporomandibular joints, including many headache sufferers. 85% of headache patients suffer from jaw misalignment and CMD, claimed a neurologist from Essen in the “Westdeutsche Allgemeine Zeitung” (Dr. Gerhard in: WAZ, 2008).
The dentist can help!
The causes of the specific functional disorder should be analyzed individually by the dentist.
Manual-clinical and instrumental functional diagnostics (DIR® concept) are available for reliable anamnesis and treatment.
In this way, you as a patient receive truly effective treatment!
Important to know!
Every patient has a right to functional prophylaxis!
It is also generally sensible and advisable to carry out a diagnostic examination with the DIR® system before fabricating new dentures in order to ensure the “correct bite” and avoid possible complications.
Schmerzen, die vom Kiefer kommen, Kopfschmerzen, Migräne, Nacken- und Schulterverspannungen, Ohrgeräusche, Tinnitus, Kiefergelenksprobleme, HWS-Beschwerden, Probleme in der Lendenwirbelsäule- alle diese Beschwerden können eine Ursache haben: CMD (Craniomandibuläre Dysfunktion). Circa acht Prozent aller Menschen leiden an der so genannten CMD. Als Craniomandibuläre Dysfunktion bezeichnet man Beschwerden, die aufgrund von Form- und Funktionsstörungen im Schädel- und Gesichtsbereich herrühren. Ein Schmerz muss seine Ursache nicht immer dort haben, wo es weh tut. Der Mensch ist eine Einheit. So passiert es oft, dass der Ursprung des Schmerzes ganz woanders zu finden ist als der Schmerz selbst. Es ist möglich, den Biss zu diagnostizieren. Eines unserer Schwerpunkte ist die Funktionsanalyse und Therapie des Kausystems. Dr. Annette Jasper, München
We are an Essen-based company that has specialized in functional diagnostics for dentists, orthodontists and dental technicians since 2006.
With the DIR® concept, we offer dentists innovative solutions for the precise diagnosis and treatment of temporomandibular joint disorders.
The concept includes manual clinical and instrumental functional analysis, on the basis of which a precise diagnosis can be made and the optimum therapy, such as the fitting of a DIR® occlusal splintcan be carried out.
The DIR® treatment pathway for the dental practice gives you confidence in functional diagnostic patient treatment.
Our central products for this are the FunktioCheck Pro® softwarefor analyzing and documenting functional diagnostic findings, and the DIR® Systemfor determining the exact mandibular positioning.
Regular training courses for dentists and dental technicians ensure that you are always working with the latest functional diagnostic possibilities.
The workflow in the laboratory and the laboratory structure are also taken into account here.
This is because it is helpful for time- and labor-saving production if the design software is not too complex so that it can be operated as intuitively as possible.
The special software tailored to this enables design directly in the plastics department.
This means that no CAD design workstations or CAD technicians are required.
Production is carried out by the same personnel who were already responsible in advance.
The simple design is supported by logical wizard steps and specific software functions tailored to the area of application.
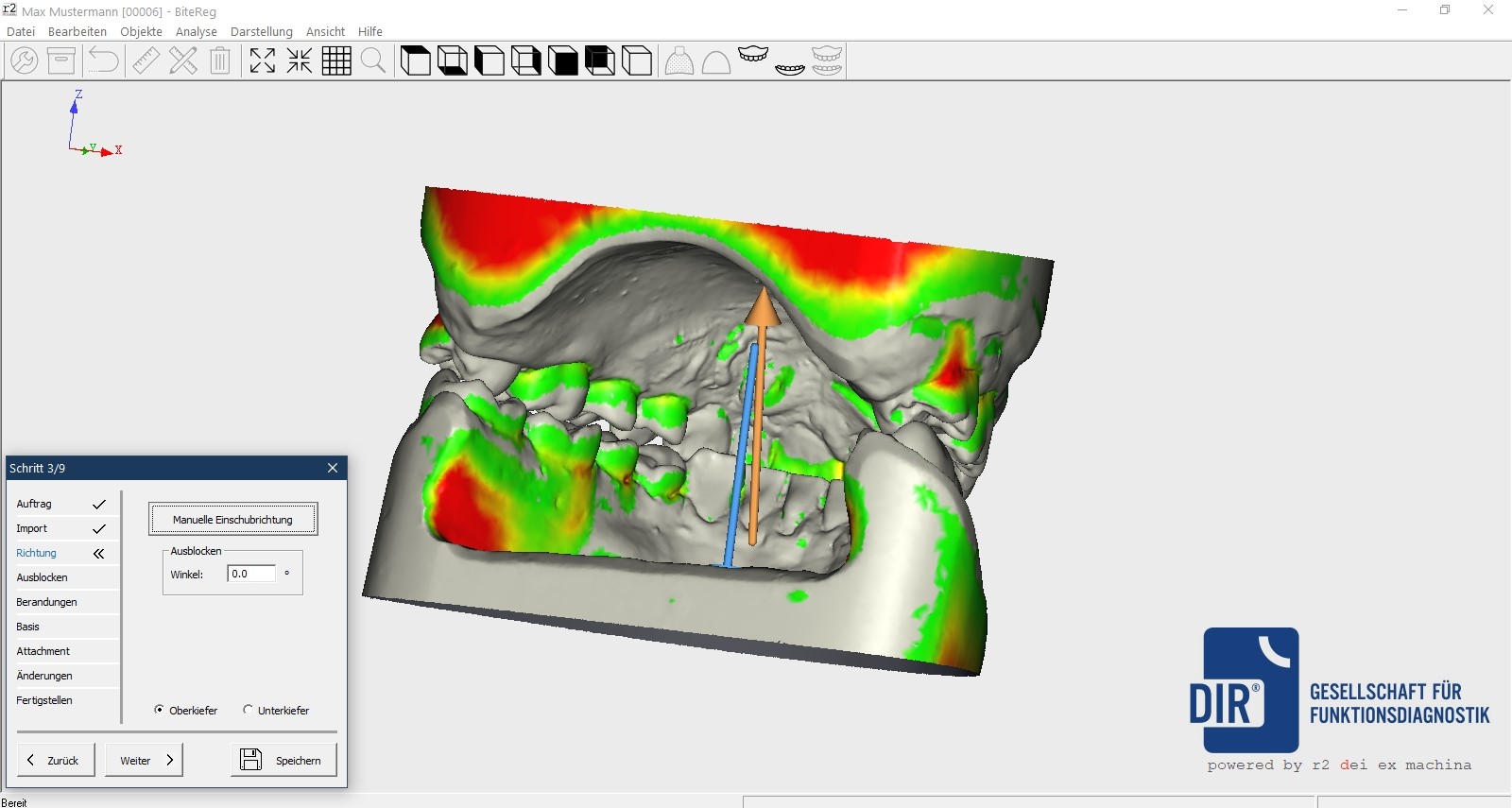
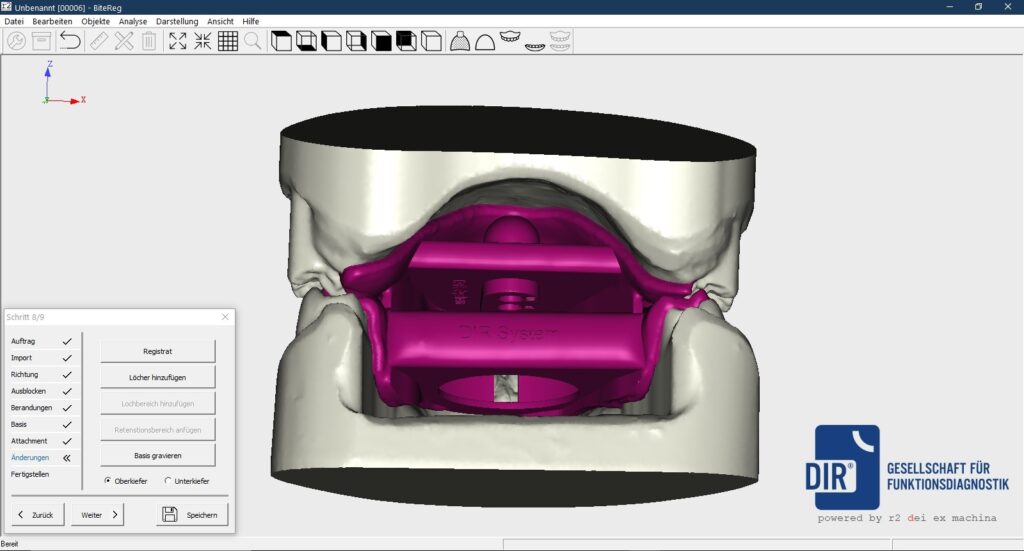
Digitization must always support the entire work process in a meaningful way… and this is what we offer you with BitReg DIR®!!!
The advantages of the digital solution at a glance:
“Easy to use” order management
Wizard-guided process, so no computer experience necessary
Simultaneous modeling OK/UK
Total and fully edged
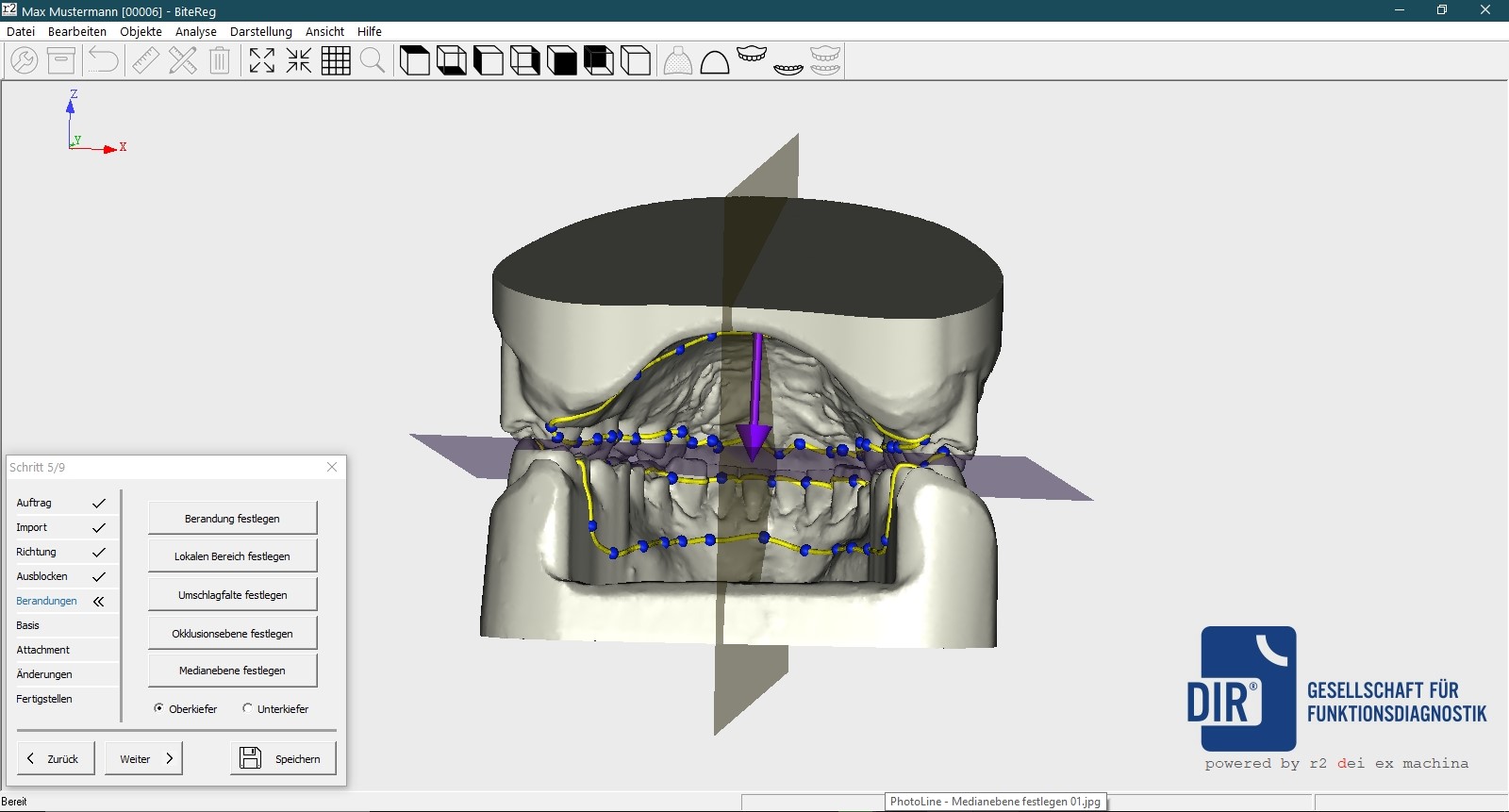
Create median level
Subsequent bite wall correction possible
Automatic bite blocking in the software
Fully automatic DIR® support pin and DIR® sensor positioning calculation
show Situ or pre-bite scan
BitReg DIR® is available exclusively from DIR® KG!
You also have the option of upgrading to the BitReg full version (creation of bite templates, set-up and functional bases and bite forks) via our cooperation partner r2.
Talk to us – Mr. Beltermann will be happy to inform you on 0201_2 79 06 09 40!
A. Dietzel1 A. Zöllner2 1Dentistry practice, Essen 2Departmentof Dental Prosthetics, Witten/Herdecke University Publication: Deutscher Ärzte Verlag, DZZ, Deutsche Zahnärztliche Zeitschrift, 2012; 67 (2)
S. Linsen, A. Samai, H. Stark, M. Klitschmüller Polyclinic for Dental Prosthodontics, Propaedeutics and Materials Science, Rheinische Friedrich-Wilhelms-Universität Bonn Publication: The Journal of Prosthetic Dentistry, Issue: Vol.
107 No 1, January 2012, p. 1-72
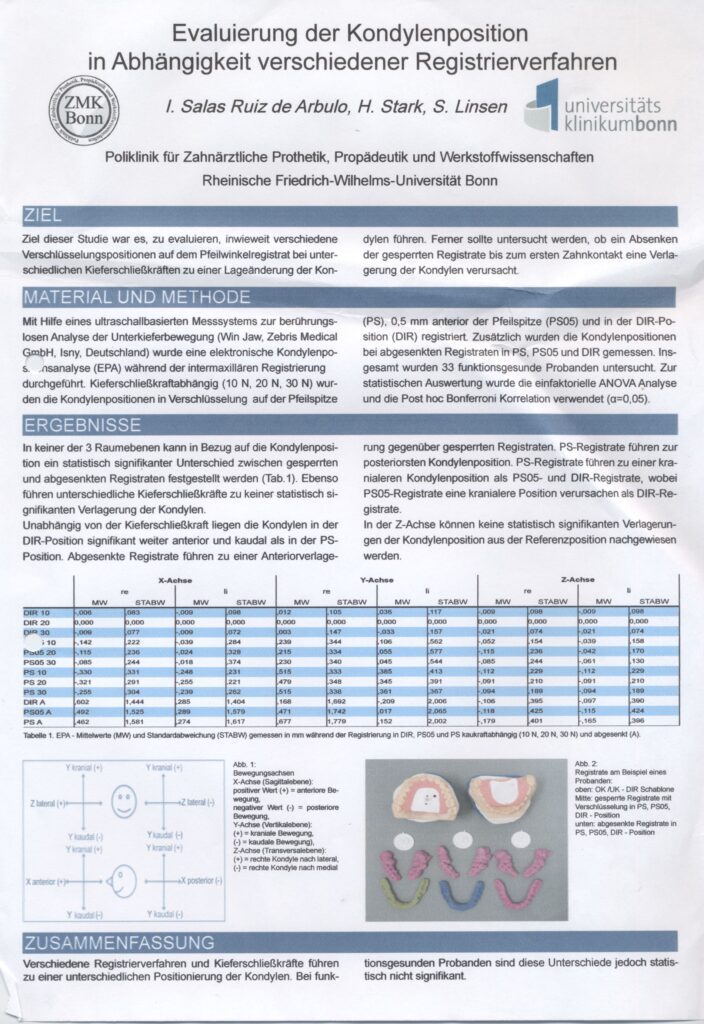
I. Salas Ruiz de Arbulo, H. Stark, S. Linsen Polyclinic for Dental Prosthetics, Propaedeutics and Materials Science, Rheinische Friedrich-Wilhelms-Universität Bonn
Philipp Scherer1, Farina Blattner2 1 Department of Oral and Maxillofacial Surgery, Klinik am Ring, Hohenstaufenring 28, 50674 Cologne 2 Practice Dr. Blattner, Gertenbachstr.
30, 42899 Remscheid
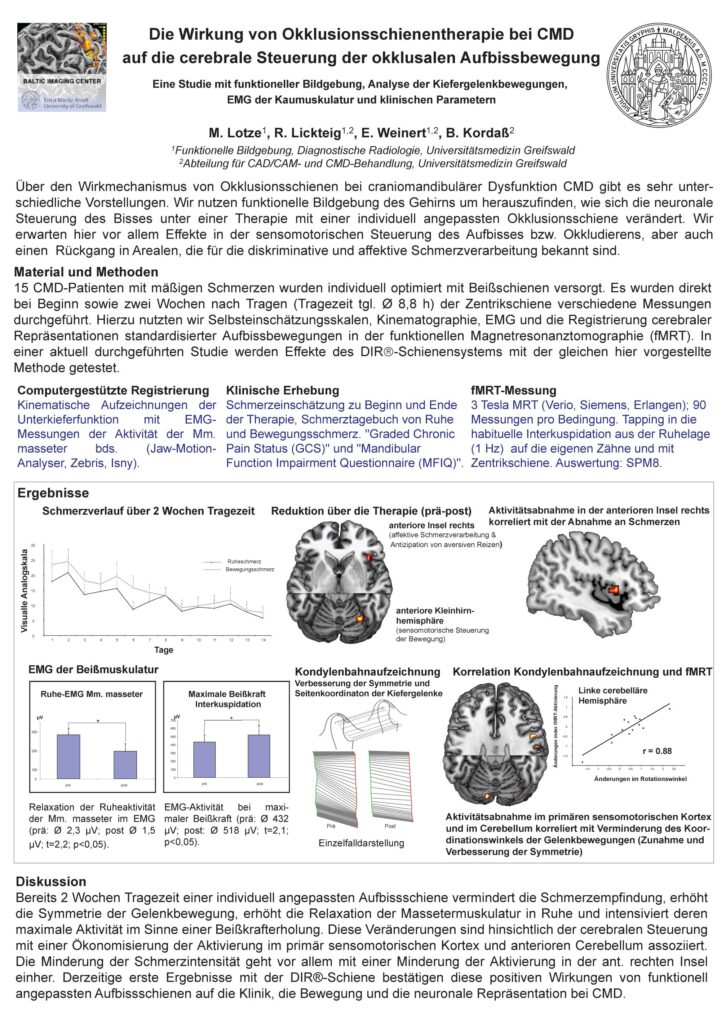
M. Lotze1, R. Lickteig1,2, E. Weinert1,2 B. Kordaß2 1FunctionalImaging, Diagnostic Radiology, University of Greifswald Department of CAD/CAM and CMD Treatment, University Medicine Greifswald
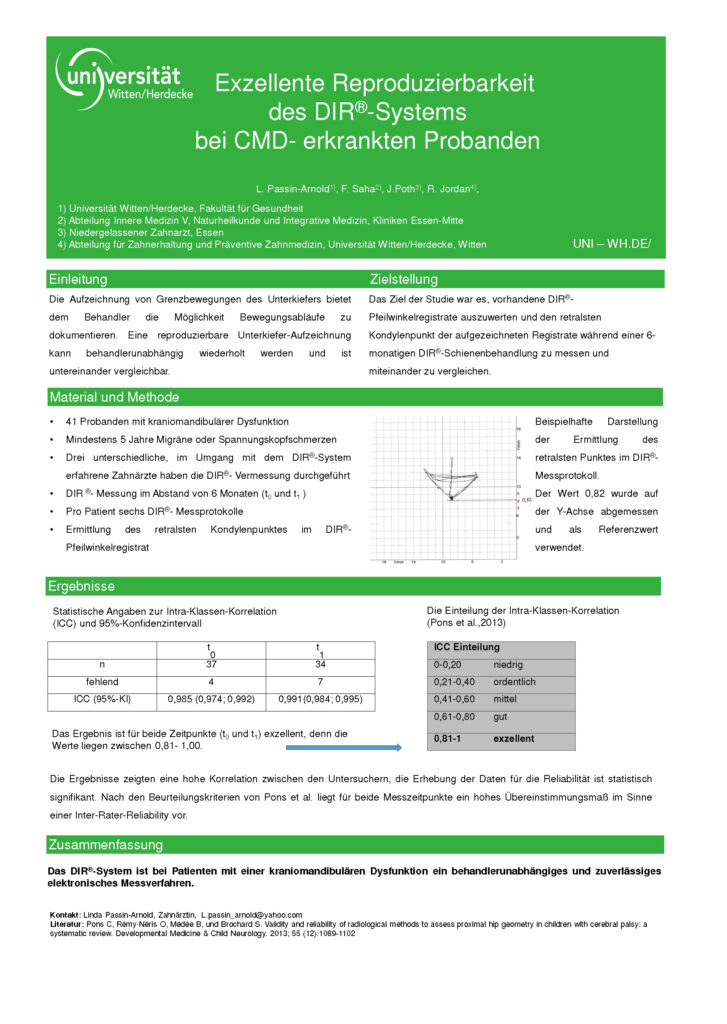
1Witten/Herdecke University, Faculty of Health – 2Department ofInternal Medicine V, Naturopathy and Integrative Medicine, Essen-Mitte Clinics 3Dentist in private practice, Essen – 4Departmentof Conservative and Preventive Dentistry, Witten/Herdecke University, Witten
Felix Joyonto Saha1, MDa, Almut Pullaa1, Thomas Ostermann, PhDb2, Theresa Millera1, Gustav Dobos, MDa1, Holger Cramer, PhD, MSc1 1Department of Inernal and integrative Medicine, Klinikum Essen Mitte, Faculty of Medicine University of Duisburg-Essen –
2Departmentof Psychology, Faculty of Health, University of Witten-Herdecke